Lay Summary
People with severely high triglycerides—blood fats at 500 mg/dL or more—face a serious risk of acute pancreatitis, a painful and potentially deadly inflammation of the pancreas. Standard treatments like fibrates or fish oil often fail to lower these levels enough and have not been proven to prevent pancreatitis attacks.
Two large international trials, called CORE-TIMI 72a and CORE2-TIMI 72b, tested a new monthly injection called olezarsen, which works by blocking a protein that traps triglycerides in the blood. The studies included over 1,000 adults, most already on other lipid-lowering drugs, with an average age of 54 and very high baseline triglycerides around 800 mg/dL. Participants were randomly assigned to receive either a 50 mg dose, an 80 mg dose of olezarsen, or a placebo shot every four weeks for one year.
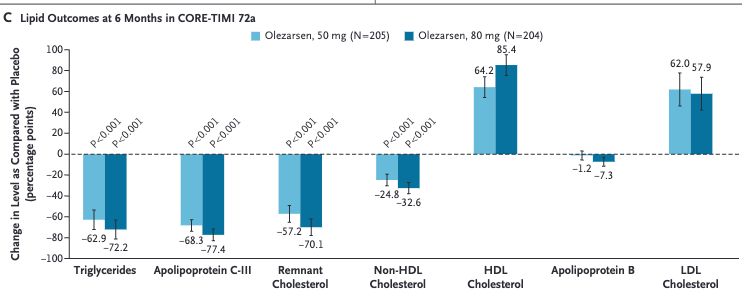
The results were striking: at six months, triglyceride levels dropped by 50 to 63 percent with the lower dose and 55 to 72 percent with the higher dose, far outperforming placebo. Beyond lowering blood fats, olezarsen dramatically reduced the risk of acute pancreatitis by 85 percent compared to placebo, with only two cases occurring in the drug groups versus 13 in the placebo group. Other harmful lipids, including remnant cholesterol and non-HDL cholesterol, also fell sharply.
While side effects were generally similar across groups, the higher 80 mg dose was linked to more liver enzyme elevations, low platelet counts, and a slight increase in liver fat.
In simple terms, olezarsen offers a powerful new way to control dangerously high triglycerides and prevent pancreatitis in people who don’t respond to usual treatments. The 50 mg dose appears to strike the best balance between strong benefits and fewer safety concerns.
Published on November 8, 2025, in the New England Journal of Medicine and funded by Ionis Pharmaceuticals, this research marks a major step forward for a hard-to-treat condition.
https://www.nejm.org/doi/full/10.1056/NEJMoa2512761
Comment
- Severe hypertriglyceridemia is a potentially serious medical condition because it can lead to recurrent attacks of pancreatitis. Preventing such attacks represents a significant unmet medical need. If multiple and severe attacks occur over time, the pancreas can be destroyed and insulin dependent diabetes can result.
- While still elevated compared to normal ranges, reducing triglyceride levels to <5.6 mmol/L (or 500 mg/dL) eliminates the risk of pancreatitis.
- Severe hypertriglyceridemia most commonly results from genetic predisposition and a contributing medical condition (diabetes, metabolic syndrome). Excessive alcohol intake can contribute. Rarely, a genetic disorder alone, namely deficiency of lipoprotein lipase or related cofactors, can lead to severely elevated triglycerides.
- Modification of diet to reduce refined carbohydrates and fats is the foundation of therapy but it can be very difficult to follow such a restrictive diet. A good website that reviews dietary interventions is https://knowyourtgs.com/fcs-nutrition-and-lifestyle.
- Use of a potent statin (rosuvastatin) and fibrates (fenofibrate is what I use in my patients to minimize drug interactions) helps to lower the triglyceride level by about 50% but it is often not enough to get below target. Icosapent ethyl (Vascepa) is purified fish oil and can also lower triglycerides by another 20-30% but the drug is expensive and can increase the risks of atrial fibrillation and bleeding slightly.
- Olezarsen is the first of a class of new drugs – Apo C3 inhibitors – that dramatically reduce triglyceride levels and pancreatitis risk. This class of medication works primarily by enhancing clearance of triglyceride rich lipoproteins. They are a welcome addition to the therapeutic armamentarium. Hopefully, pricing won’t limit access, but it probably will.
- Because elevated triglyceride remnants are also a risk factor for cardiovascular disease, there is interest in use of these drugs for cardiovascular disease prevention but no randomized trials are available yet. One issue is that these drugs cause LDL (low density lipoprotein) cholesterol levels to increase (by about 1.0-1.5 mmol/L or 37-62 mg/dL in these two studies) and it remains to be seen if this has a detrimental effect on cardiovascular disease incidence. However, the reason why LDL-C is increasing is because the triglycerides rich particles are being appropriately cleared and this leads eventual conversion to LDL in the circulation.
- The increase in liver steatosis, liver enzymes, and decrease in platelet counts seen primarily with the 80 mg dose require monitoring and further study. The 50 mg dose has a better risk-reward profile.

Leave a comment